
Between 1998 and 2008, spinal fusion surgery (a form of back surgery) had increased 2.4-fold in the United States.(1) And the most common reason for the increase? Disc degeneration.(2) Back surgery has its place and time, but opting for one is not a small decision. It’s also a procedure that cannot be undone. Asking yourself the following questions will help you make an informed decision.
-
Does degeneration and disc herniation automatically warrant a surgery?
The short answer is NO. Although degeneration, bone spurs and disc herniations can look alarming on x-ray and MRI, they are not always relevant to one’s pain and dysfunction. In fact, a 2015 review (3) says what you see on your films most likely has nothing to do with your pain. In other words, pain, along with degenerative changes, are not good enough reasons for back surgery. Read more about this topic here.
-
When to consider surgery for back and leg pain?
Although there are spinal emergencies that need immediate surgical evaluations, sciatica caused by herniated disk or spinal stenosis ALMOST NEVER requires back surgery. (4) It is known that even patients with a massive disc herniation can do very well under conservative treatment. (5)
If you have leg pain without neurological symptoms, then you should be treated conservatively. (6) Having a negative straight leg raise test means surgery most likely won’t work for you. (7) If you have sciatica, you are over 40, and you have severe leg pain, surgery probably won’t work for you. (8) When your MRI only shows a little compression on the nerve, you likely will do worse after surgery. (9) Most patients with chronic low back pain will NOT benefit from surgery. (10)
Surgery may be appropriate when you have
- severe or worsening neurological deficits (4) OR
- leg pain that is worse than back pain AND positive straight leg raise test AND none-responsive to conservative therapy in 4-12 weeks AND imaging correlates with the symptoms. (4)
-
Does back surgery have superior results compared to conservative care?
So far, most of the studies available to answer this question are low quality studies. The consensus is that long-term results of back surgery are NOT superior to conservative treatment. (8,11,12) As of 2016, back surgery cannot be confidently recommended for lumbar spinal stenosis, because it doesn’t provide better outcomes, and the side effects are much higher than conservative treatment (24% vs. 0%). (13)
On average, one year after having a low back discectomy for disc herniation, a quarter of the patients have another herniation at the same level that received the surgery. (14) 22% patients have worsening low back pain in a year, and recurrent low back pain is as high as 36% among these people. (15)
Fusion surgery is in your favor if you have a large compression onto the space surrounding the spinal cord, specifically greater than 1/3 thecal sac compression. (9) However, 1 out 10 patients will be operated on again in a couple years, and 1 out of 5 will be operated on again in 10 years. (16) Basically, the studies are saying patients do pretty well after the fusion surgery…the outcomes are good…except that a good portion of them will have to come back and get the surgery again in the future. (17) So therefore, make sure it’s risk you are willing to take if surgery is what you opt for.
The Bottom Line
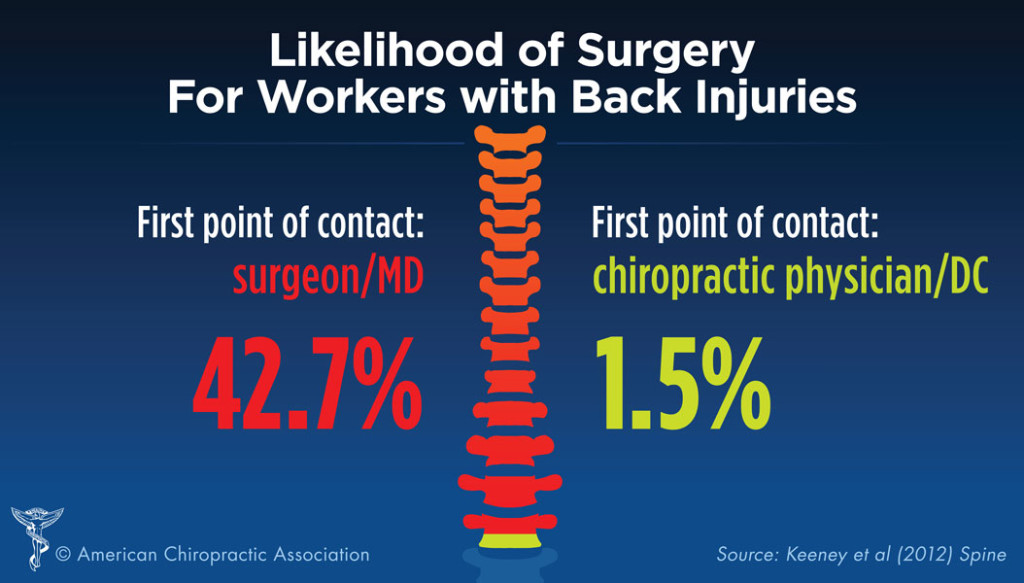
If you have back pain and you visit a surgeon, there is a good chance you will end up having back surgery, as demonstrated by a 2013 study. (18) (see graphic below). If you see a chiropractor first, there is a good chance you will avoid the back surgery that may not be necessary in the first place.
The bottom line is if you are experiencing back pain, find a good chiropractor who is familiar with the research, who knows what to look for, who knows how to check for the different indicators and neurological signs, and recommend care (surgical or not) based on existing evidence.
References:
- Rajaee SS, Bae HW, Kanim LE, Delamarter RB. Spinal fusion in the United States: analysis of trends from 1998 to 2008. Spine. 2012 Jan 1;37(1):67-76. [PubMed]
- Cowan JA Jr, Dimick JB, Wainess R, Upchurch GR Jr, Chandler WF, La Marca F. Changes in the utilization of spinal fusion in the United States. Neurosurgery. 2006 Jul;59(1):15-20. [PubMed]
- Brinjikji W, Luetmer PH, Comstock B et al. Systematic literature review of imaging features of spinal degeneration in asymptomatic populations. AJNR Am J Neuroradiol. 2015 Apr;36(4):811-6. [PubMed]
- Atlas SJ, Deyo RA. Evaluating and managing acute low back pain in the primary care setting. J Gen Intern Med. 2001 Feb; 16(2):120-31. [PubMed]
- Benson RT, Tavares SP, Robertson SC, Sharp R, Marshall RW. Conservatively treated massive prolapsed discs: a 7-year follow-up. Ann R Coll Surg Engl. 2010 Mar;92(2):147-153. [PubMed]
- Atlas SJ, Nardin RA. Evaluation and treatment of low back pain: an evidence-based approach to clinical care. Muscle Nerve. 2003 Mar;27(3):265-84. [PubMed]
- Sedighi M, Haghnegahdar A. Lumbar disk herniation surgery: outsome and predictors. Global Spine J. 2014 Dec;4(4):233-244. [PubMed]
- Lequin MB et al. Surgery versus prolonged conservative treatment for sciatica: 5-year results of a randomized controlled trial. BMJ Open 2013;3:e002534. [BMJOpen]
- Lurie JD et al. Magnatcie resonance imaging predictors of surgical outcome in patients with lumbar intervertebral disc herniation. Spine. 2013 Jun 15;38(14):1216-25. [PubMed]
- Last AR, Hulbert K. Chronic low back pain: evaluation and management. Am Fam Physician. 2009 Jun 15;79(12):1067-74. [PubMed]
- Schoenfeld AJ, Weiner BK. Treatment of lumbar disc herniation: evidence-based practice. Int J Gen Med. 2010;3:209-214. [PubMed]
- Jacobs WCH et al. Surgery versus conservative management of sciatica due to a lumbar herniated disc: a systemic review. Eur Spine J. 2011 Apr;20(4):513-522. [PubMed]
- Zainea F et al. Surgical versus non-surgical treatment for lumbar spinal stenosis. Cochrane Database Syst Rev. 2016 Jan 29;1:CD010264. [PubMed]
- Lebow RL et al. Asymptomatic same-site recurrent disc herniation after lumbar discectomy: results of a prospective longitudinal study with 2-year serial imaging. Spine. 2011 Dec 1;36(25):2147-51. [PubMed]
- Parker SL et al. Incidence of low back pain after lumbar discectomy for herniated disc and its effect on patient-reported outcomes. Clin Ortho Relat Res. 2015 Jun;473(6):1988-99. [PubMed]
- Kim CH et al. Reoperation rate after surgery for lumbar spinal stenosis without spondylolisthesis: a nationwide cohort study. Spine J. 2013 Oct;13(10):1230-7. [PubMed]
- Liang L, Jiang WM, Li XF, Wang H. Effect of fusion following decompression for lumbar spinal stenosis: a meta-analysis and systematic review. Int J Clin Exp Med. 2015;8(9):14615-14624. [PubMed]
- Keeney BJ, Fulton-Kehoe D, Turner JA, Wickizer TM, Chan KC, Franklin GM. Early predictors of lumbar spine surgery after occupational back injury: results from a prospective study of workers in Washington State. Spine. 2013 May 15;38(11):953-64. [PubMed]
About the Author
Dr. Lily Semrow is a Board Certified Chiropractic Neurologist who focuses on Neuro-Structural Correction. She has a B.S. in Nutrition and a doctorate in Chiropractic. She has a passion for serving families, and helping people who could not get better through traditional and alternative means.
Comments 4
I like that you mention that herniated discs almost never require back surgeries. When it comes to herniated discs, it’s good that there are a variety of treatment options. My dad just hurt his back with a herniated disc, so he’s looking to see which treatment option would be best for him.
Author
Glad you liked the article Cameron. Thanks for the feedback! I hope your Dad finds the help he needs.
I think that you make a good point that you should get spine surgery if your leg pain is worse than your back pain or if you have worsening problems. It’d probably be most important to find a doctor or surgeon who knows what their doing and can tell you exactly what will be best for you. If they said that it would be best you get operated on, then you’d want to find somewhere to get spine surgery.
Author
Glad you liked the article Amanda! Yes, surgery may be warranted under certain conditions, but pain by itself is often not a good reason. Conservative care goes a long way if you find the right doctor. A knowledgeable chiropractor will also know when surgery may be needed and refer for surgical consultation.